A new case report published by David B. Clifford, MD, and colleagues detailed the anti-amyloid therapy treatment course of a patient who developed Alzheimer’s disease concurrently with a pre-existing HIV diagnosis. The patient, who was diagnosed with HIV in 2005, began showing signs of cognitive decline in 2015 and received a clinical diagnosis of Alzheimer’s disease in 2024, after which he was started on anti-amyloid therapy. With promising post-treatment cognitive test results in this first patient, the authors called for further investigations on the safety and efficacy of anti-amyloid therapy treatments for people living with HIV.
There has been incredible progress in Alzheimer’s disease research in recent years, from blood-based biomarker tests for detecting Alzheimer’s disease and measuring disease progression to FDA-approved therapies that have been shown to slow down the progression of Alzheimer’s disease in some patients by removing some of the amyloid plaque buildup in the brain. However, in all documented clinical trials of anti-amyloid therapies to date, people living with HIV were excluded from trial populations, despite lack of evidence suggesting that anti-amyloid therapy should not be combined with HIV therapy.
The case study by Clifford and colleagues — the first published case report on anti-amyloid therapy in a person living with HIV — represents a meaningful first step in filling a crucial gap in clinical trials related to Alzheimer’s disease therapeutics. The study’s findings suggest that people living with HIV may be good candidates for anti-amyloid therapy if they develop the usual clinical indicators of Alzheimer’s disease.
In untreated AIDS, a common comorbidity was a progressive dementia that often led to death within six months of onset. With the development of a remarkable combination anti-retroviral therapy that controls the infection, this form of dementia has become rare in those receiving treatment. However, with more and more people living with the human immunodeficiency virus well into their senior years, there has been a concomitant increase in Alzheimer’s disease and other age-related dementias developing in people living with HIV.
“Having come so far in developing remarkably effective therapy for HIV, we are committed to also providing the best care for other complications that develop with aging. Too often, people living with HIV have been excluded in the development of therapy, making it harder to provide optimal care.”
David B. Clifford, MD
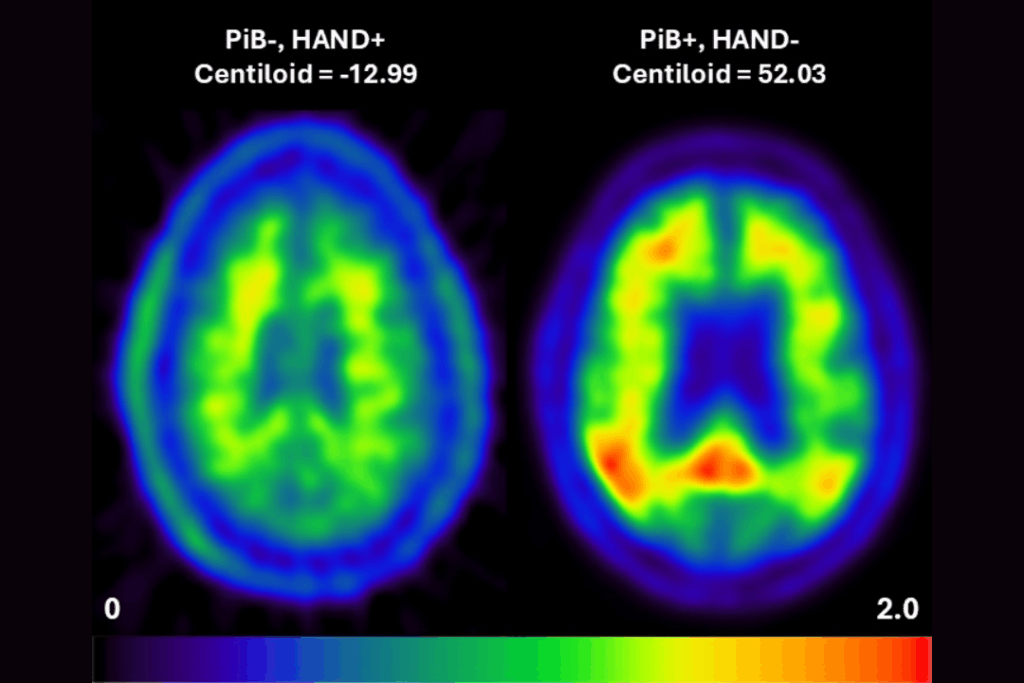
HIV-associated neurocognitive disorder (HAND) has emerged as a frequent complication for those who are undergoing treatment for HIV. However, HAND is a generally non-progressive form of impairment, unlike Alzheimer’s disease and related dementias. It also does not replicate the usual indicators of Alzheimer’s disease, such as amyloid build up in the brain or certain biomarkers in the cerebrospinal fluid. Clifford’s case report suggests that HAND and Alzheimer’s disease in people living with HIV require different testing and treatment approaches.
Clifford, the Melba & Forest Seay Professor of Clinical Neuropharmacology in Neurology and section chief of Neuroinfectious Diseases at Washington University School of Medicine in St. Louis, is a world-renowned expert in HIV-related neurological conditions and has also long been involved with the Knight Alzheimer Disease Research Center (ADRC) at WashU Medicine. Combining his two areas of expertise, Clifford and his colleagues treated a 72-year-old patient who had been undergoing treatment for HIV since 2005 and whose 2024 lumbar puncture showed results consistent with an Alzheimer’s disease diagnosis.
After fully informing the patient of potential risks as well as conducting a special risk assessment, Clifford’s team began the patient on a standard treatment protocol of lecanemab, an FDA-approved antibody infusion therapy that has been shown to reduce the accumulation of beta-amyloid in the brain and improve cognitive and functional symptoms for individuals in the earlier stages of Alzheimer’s disease. After 11 months on the therapy, Clifford’s patient showed stable or even slightly improved scores on cognitive tests and did not experience any of the known side effects of anti-amyloid therapies. His HIV continued to be managed successfully with his usual protocol while undergoing anti-amyloid treatment. Based on these promising outcomes, the authors called for additional studies investigating the use of anti-amyloid therapies in people living with HIV.
“We are delighted that this first step in introducing the latest therapy for Alzheimer disease appears to be possible while still maintaining the benefits of HIV therapy,” Clifford said. “We look forward to sharing this information with caregivers seeking to optimize care in an aging HIV population and expanding the experience with this therapy in future studies of this population.”
Clifford DB, Benzinger TLS, Han JY, Powles S, Paczynski M, Ances BM, Campbell JW. Treating Alzheimer’s disease in a person living with HIV. Alzheimers Dement (Amst). 2026 Feb 17;18(1):e70259. doi: 10.1002/dad2.70259. PMID: 41717085; PMCID: PMC12914134.